|
|
|
|
|
|
Location of tumor, posterior thigh |
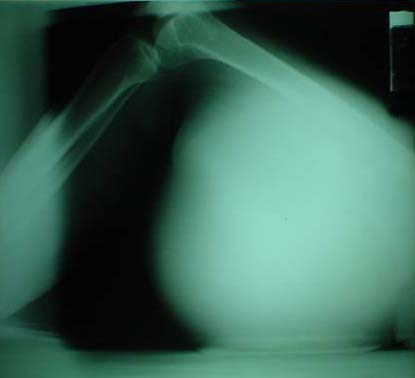
X-ray of the thigh, lateral view |
X-ray of the thigh, AP view |
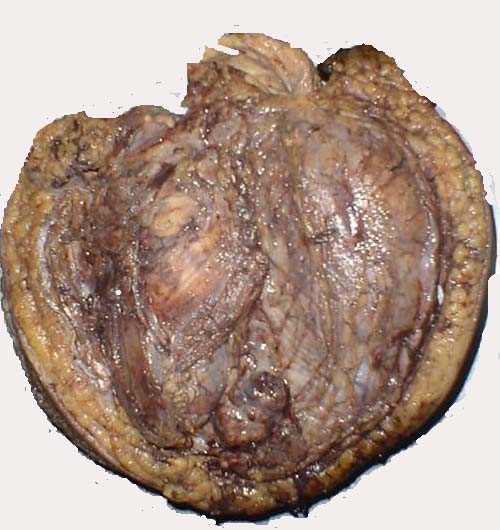
Formalized specimen |
Tetanus in a Necrotic Soft Tissue Sarcoma of the Lower Extremity
Ana Maria G. Agoo-Llado, MD
Jose Ravelo T. Bartolome, MD, FPCS
Reynaldo O. Joson, MD, MHA, MHPEd, MS Surg
Department of Surgery
Ospital ng Maynila Medical Center
2002
SUMMARY:
A Filipino patient with a necrotic soft tissue sarcoma who developed tetanus was presented to instill awareness that tetanus can occur in tumors and not just in traumatic wounds. A review of literature was made which showed that, though uncommon, tetanus could occur in tumors, especially in those with necrosis. Low oxygen potential in the growing tumor compounded by contamination with clostridium tetani spores and possibly endogenous reactivation of latent tetanus bacteria has been hypothesized as the principal mechanism. Recommended preventive measures include early treatment of the tumor before necrosis sets in and when necrosis has occurred, early treatment, usually by surgical extirpation, if possible, and anti-tetanus prophylaxis.
INTRODUCTION:
Tetanus usually is associated with traumatic wounds. Rarely, is it associated with tumors.
The global incidence of tetanus is though to be about 1 million cases annually. The US centers for Disease Control and Prevention receive reports of about 70 domestic cases per year; this represents underreporting of about 60%.1 Acute injuries (punctures and lacerations) account for 70% of cases, other identifiable conditions are noted in 23%, 7% of cases without an apparent source.2 Unreported cases of tetanus may include patients with the infection without an obvious point of entry or patients with unusual source and site of infection. This population may include patients with malignant necrotic tumors.
In the Philippines, the exact incidence of tetanus in patients with tumors, particularly malignancies, is not known but is felt to be uncommon if not rare. The authors have not encountered any published case report on topic in the local literature. Thus, this case report with the goal of informing physicians, other health care givers as well as the public that tetanus can occur in a soft tissue sarcoma or any malignancy and tumor for that matter, and therefore, the need for early preventive measures.
CASE REPORT:
A 30-year-old female had a malignant soft tissue sarcoma (fibrosarcoma) of the right lower extremity, on the posterior aspect of the thigh for about 2 years prior to consult. The mass had grown to occupy the entire posterior thigh, with necrotic areas. There was no involvement of the bone and neurovascular bundle. While at the ward, she experienced generalized tetanus, manifested by rigidity of the masseter muscles (trismus) followed by neck rigidity, opisthotonus and paroxysmal, violent muscle spasms. Tetanus was entertained based on clinical manifestations. As soon as diagnosed, she was given tetanus immunoglobulin, tetanus toxoid, penicillin G, metronidazole and diazepam. The patient underwent stat debridement with wide excision of the tumor. Respiration was supported with a mechanical ventilator. However, the patient's condition deteriorated despite the management.
Location of tumor, posterior thigh
X-ray of the thigh, lateral view
X-ray of the thigh, AP view
Formalized specimen


DISCUSSION:
It is important to consider a necrotic soft tissue tumor as a tetanus prone wound like in injuries sustained by trauma. The pathophysiology of tetanus developing in a soft tissue sarcoma of the extremity can be explained in the following way:
In a solid tumor like a soft tissue sarcoma, oxygen can diffuse radially from capillaries for only 150 - 200 um. When distances exceed this, cell death follows and necrosis occurs. Thus, a tumor undergoes necrosis or ulceration when cell division outgrows vascular supply. The hypoxic necrotic region then provides optimal conditions for growth of anaerobic clostridia. Experimental injection of spores of Clostridium tetani can cause tetanus in mice with necrotic malignant tumors 3.
The abovementioned basic pathophysiology probably holds true for any surface tumor that develops tetanus - low oxygen potential in the growing tumor complicated with contamination by Clostridium spores either from the soil or dust. Endogenous reactivation of latent tetanus bacteria has been implicated as a cause beside direct contamination.
Review of world literature shows a number of tetanus developing in tumors, both superficial and deep ones.
Stassen, et al 4 reported a patient with a T3NxM0 esophageal cancer who later developed tetanus infection. He suggested that in this patient with no visible external wound, the esophageal mucosal cancer lesion could have served as a portal of entry or that endogenous reactivation of latent tetanus bacteria had taken place.
Earist, et al, 5 reported a case in a previously immunized patient who was exposed to the dust of old building plaster containing horse hair. The site of infection was a squamous cell cancer of the scalp.
Coulson, et al, 6 had a patient with tetanus in a necrotic 5 kg leiomyoma of the uterus. He stated that there are 2 other cases of uterine tetanus other than in a post-abortal tetanus.
Johkura, et al, 7 in 1999, reported a tetanus case originating from a benign scalp tumor showing that a benign neoplasm of the skin, in this case, a solitary trichoepithelioma, can be predisposed to clostridial infection.
Karnad 8 reported seven cases: 50 year old man with an ulcerated squamous cell carcinoma on the posterior third of his tongue; 50 year old female with an ulcerating adenocarcinoma of the breast of 3 months duration; patient 3 developed mild tetanus the day after biopsy of an ulcerated breast lesion; patient 4, a 50 year old woman with a squamous cell carcinoma of the mucosa of her left cheek; patient 5 had an ulcerated metastatic cervical lymph node; patient 6 had a well-differentiated carcinoma of the oropharynx undergoing chemotherapy; patient 7 , a postmenopausal woman with an ulcerated squamous cell carcinoma of the cervix. He also reposrted an association between colorectal cancer and clostridial myonecrosis. In his review of 55 such cases, all had necrotic tumors, and 35% had occult cancer that was detected only after they developed myonecrosis 9 .
Tetanus is preventable in almost all patients leading to its description as the "inexcusable disease". This statement should not be confined to traumatic wounds only. It should be applied to necrotic tumors as well, now that awareness has been made that tetanus can occur in such a situation.
The primary preventive measure against tetanus developing in tumors should be early treatment of the tumor before necrosis sets in. Thus, early consult should be emphasized to the public. Once necrosis sets in, the primary preventive measure against tetanus should be early removal of the necrotic tumor if possible, usually by surgical extirpation, and the secondary preventive measure is to administer anti-tetanus prophylaxis. The standard regimen recommended for anti-tetanus prophylaxis in traumatic wounds can be used. Once tetanus has developed, appropriate management should be instituted with the following goals in mind: eliminate the source of toxin; neutralize unbound toxin; prevent muscle spasms; and provide support to certain organ systems.
SUMMARY:
A Filipino patient with a necrotic soft tissue sarcoma who developed tetanus was presented to instill awareness that tetanus can occur in tumors and not just in traumatic wounds. A review of literature was made which showed that, though uncommon, tetanus could occur in tumors, especially in those with necrosis. Low oxygen potential in the growing tumor compounded by contamination with clostridium tetani spores and possibly endogenous reactivation of latent tetanus bacteria has been hypothesized as the principal mechanism. Recommended preventive measures include early treatment of the tumor before necrosis sets in and when necrosis has occurred, early treatment, usually by surgical extirpation, if possible, and anti-tetanus prophylaxis.
REFERENCES:
1. Sutter RW, Cochi SL, Brink EW, Sirotkin BI. Assessment of vital statistics and surveillance data for monitoring tetanus mortality, United States, 1979-1984. Am J of Epidemiol. 1990:131:132-142.
2. Bleck TP. Tetanus: Dealing with the continuing clinical challenge. J Crit Illness 1987; 2:41-52.
3. Mahagren RA, Flanigan CC. Localization of the vegetative form of Clostridium tetani in mouse tumors following intravenous spore administration. Cancer Res. 1955; 15:473-8.
4. Stassen PM, Koppjan EH, Van Dijke BJ, Wirtz, JJ: A patient with tetanus without an obvious point of entry. Ned Tschr Geneeskd 142(43):2361-3, 1998.
5. Earist JE, Hillis AN, MaCaulay MB: J. Infect 7 (1): 72-73, 1983.
6. Colson AS, Lee H: Tetanus in a patient with a uterine tumor. Am Surg 42(3): 215-8, 1976.
7. Johkura K, Kuroiwa Y, Hara M: Journal of Neurology, Neurosurgery and Psychiatry; London; 67(1):120-1, Jul 1999.
8. Karnad DR, Tilve GH. Tetanus from ulcerated tumor. Ann Intern Med 1990 Jul 15:113 (2): 170-1.
9. Kornbluth AA, Danzig JB, Bernstein LH. Clostridium septicum infection and associated malignancy. Medicine (Baltimore). 1989;69:30-7.
10. Brennan, MF: Soft Tissue Sarcoma. In: CANCER Principles & Practice of Oncology. DeVita, et.al. (ed). Philadelphia: Lippincott Williams & Wilkins, 2001, p. 1841-1890.
11. Enzinger, FM: Soft Tissue Tumors; 3rd Edition, 1995.