Swallowed Barbeque Stick Causing Surgical Abdomen
Maria Cecilia T. Leyson, MD
Harry Go, MD, FPCS
Reynaldo O. Joson, MD, MS Surg
Department of Surgery
Ospital ng Maynila Medical Center
Swallowed Barbeque Stick
ABSTRACT
A Filipino patient who swallowed a 5-cm barbeque stick and then developed surgical abdomen secondarily to perforated intestine (cecum) is being reported to create awareness among health professionals and the public of the potential of swallowed barbeque stick causing a surgical abdomen. Discussion focused on circumstances how barbeque stick can be ingested (during drinking spree), the dire consequences (intestinal perforations), how to avoid such a situation (remove barbequed foods from the stick and eat from a plate), and what to do when a barbeque stick is swallowed (close monitoring for adverse event and early medical professional consult).
Key Words: Barbeque stick, foreign bodies in gastrointestinal tract
__________________________
Reprint Request: Maria Cecilia T. Leyson, M.D.
Department of Surgery, Ospital ng Maynila Medical Center
INTRODUCTION
A barbeque stick is a slender piece of wood, usually a bamboo, about one foot long, with one pointed end used to skewer chunks of food which will be cooked over burning charcoals. Ingestion of even a portion of barbeque stick is very unusual with no report of such incident encountered during search of medical literature. Ingested foreign bodies reported that approximate the physical nature of the barbeque stick are wood splinters, toothpicks, and pencils (1-6).
This is a case report of a Filipino patient who developed an acute surgical abdomen after swallowing a portion of a barbeque stick.
There are two reasons why this case report is being made. One is for the benefit of the health professionals - to make them aware that swallowing barbeque stick is a potential cause for surgical abdomen. Awareness will facilitate early and correct diagnosis and early treatment thereby promoting successful patient management. Two is for the benefit of the public - to make them aware that swallowing barbeque stick is a potential cause for surgical abdomen. Awareness will promote avoidance of swallowing of barbeque sticks thereby reducing the incidence of surgical abdomen related to such event and its attendant mortality and morbidity consequences.
CASE REPORT
A 36-year-old Filipino male consulted Ospital ng Maynila Medical Center with a chief complain of right lower quadrant abdominal pain. His condition started one day prior to consult when he experienced a right lower quadrant abdominal pain, characterized as colicky, tolerable, non-radiating, and not relieved nor aggravated by food intake, and with no other associated signs and symptoms. No medications were taken. The pain increased in severity after a few hours. It became continuous and intolerable. There was no history of anorexia, vomiting, changes in bowel movement, dysuria, hematuria and fever.
General examination revealed a moderately built man. Physical examination findings were normal except for the abdomen, which revealed a direct and rebound tenderness at the right lower quadrant. He was diagnosed to have acute appendicitis and was operated on after three hours.
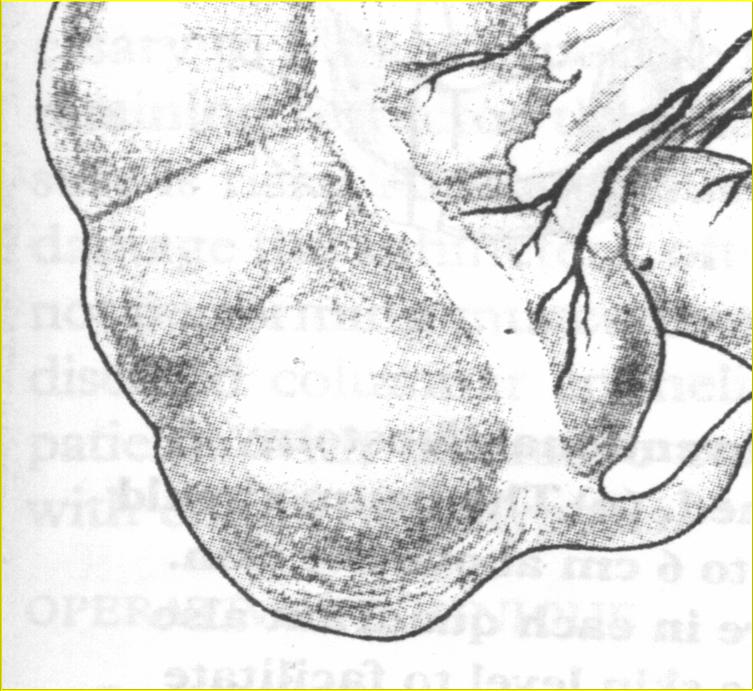
Intraoperatively, after doing a transverse right-lower-quadrant abdominal incision, what was seen was a 5-cm barbeque stick perforating the lateral aspect of the cecum, opposite the ileocecal valve, near the anterior taenia and about 7 cm from the base of the appendix. Erythema and fibrin materials were noted around the perforation. The appendix was grossly normal.
Figure 1. Where the tip of the bamboo stick perforates the cecum
Figure 2. The barbeque stick

The barbeque stick was then pulled out through the cecal perforation. Debridement and primary repair of the perforation were done. The appendix was removed.
Postoperative course was uneventful. The patient was discharged after three days. Oral medications were continued at home. He was advised to come back after one week for follow-up and suture removal.
After the operation, the patient was asked if he remembered swallowing a splinter of a barbeque stick. Although he said no, he remembered eating barbeque while having a drinking spree with his friends, three days before the onset of symptoms.
DISCUSSION
Foreign body ingestion as a whole is quite common (1-6), but swallowing a barbeque stick is very unusual. Search of Medline and Internet did not yield any report on swallowed barbeque stick. Reported foreign bodies ingested that resemble the physical characteristics of barbeque sticks are toothpicks, wood splinters, and pencils (1-16).
Exchange of information with surgical colleagues at OMMC revealed encounter of three other cases who had ingested barbeque stick splinter in the last 5 years. The 3 patients complained of anal pain whose investigation eventually led to the discovery of a part of a barbeque stick being impacted in the rectal area. The sticks were manually removed without the need for a celiotomy.
Swallowing a portion of barbeque stick can either be unintentional or intentional, as is the case in ingestion of other foreign bodies. Likewise, the usual circumstances that contribute to foreign body swallowing or ingestion in general may also be seen in barbeque stick ingestion, which include presence of psychiatric disorders, mental retardation, and mental impairment due to alcohol and drugs (5).
In the case reported and in the 3 cases shared by colleagues, all had history of a drinking spree and eating barbequed foods on a stick. Presumably, there was impairment of the mental awareness at least due to alcohol that led to the accidental swallowing of a portion of a barbeque stick. Use of drugs concomitant with alcohol could not be totally discounted.
Once swallowed, foreign bodies may or may not cause adverse events. Most of the time, the foreign bodies will pass out spontaneously. About 15-35% will cause complications like impaction, obstruction and perforations (17). Sharp and pointed objects as well as elongated foreign bodies were commonly associated to intestinal perforation.
The complications of ingested foreign bodies usually occur at sites of narrowing, such as the pylorus, the ligament of Treitz, the ileocecal valve, and the rectosigmoid junction. A retrospective study by Pinero et al. concluded that the most common site of perforation were the ileocecal valve and the rectosigmoid area (18). McManus (19) reported the terminal ileum to be one of the more common sites for obstruction and perforation to take place especially by objects with two sharp, pointed ends and about 9% of perforation were due to wood splinters, toothpicks or pencils.
The mortality and morbidity rates of patients undergoing operation for surgical abdomen resulting from swallowed barbeque sticks and ingested foreign bodies in general are usually dependent on the time of consult and treatment. Late consult and treatment are usually associated with a high mortality and morbidity rate.
The crucial factor in minimizing mortality and morbidity rates in patients who develop a surgical abdomen as a result of a swallowed barbeque stick is early recognition of any accompanying adverse event, usually impaction, obstruction or perforation. To enable early recognition of an adverse event, the public and health professionals should first realize that barbeque stick, usually a portion of it, though unusual, can be accidentally swallowed during times of mental awareness impairment especially during a drinking spree.
For the health professionals, at present, swallowed barbeque stick is not included as a differential diagnosis in patients presenting with surgical abdomen, primarily because of the absence of awareness of its occurrence and the rarity of the event. With this case report and the 3 informal cases, in a patient presenting with an acute surgical abdomen after a drinking spree and with a history of eating barbequed foods (which in the Philippines are skewered in a barbeque stick), swallowed barbeque stick should be included as one of the differential diagnoses.
The public should be advised on the occurrence of such event and the danger of swallowing barbeque stick especially during a drinking spree and when the foods served are on barbeque sticks. An advice on primary prevention of accidental swallowing will be to remove the foods from the barbeque sticks after cooking and just to eat the barbequed foods from a plate.
The public should also be advised on what to do when barbeque sticks are accidentally ingested or swallowed. This is part of a secondary preventive measure along the line of avoiding undue mortality and morbidity. Persons who accidentally swallowed barbeque stick should closely monitor themselves for abdominal pain which could be a signal of adverse event setting in. Once abdominal pain is present, they should consult right away an abdominal surgeon (usually with the title of general surgeon) who will advice them accordingly, whether to continue to monitor for adverse events or in case an adverse event has occurred, what type of treatment needs to be instituted.
SUMMARY
A Filipino patient who swallowed a 5-cm barbeque stick and then developed surgical abdomen secondarily to perforated intestine (cecum) is being reported to create awareness among health professionals and the public of the potential of swallowed barbeque stick causing a surgical abdomen. Discussion focused on circumstances how barbeque stick can be ingested (during drinking spree), the dire consequences (intestinal perforations), how to avoid such a situation (remove barbequed foods from the stick and eat from a plate), and what to do when a barbeque stick is swallowed (close monitoring for adverse event and early medical professional consult).
REFERENCES
1. Cossavella D, Clerico G, Paino O, Pozzo M, Trompetto M. Intestinal perforation caused by a toothpick. Minerva Chir 1998; 53(3):219-22.
2. Hewett PJ, Young JF. Toothpick injuries to the gastrointestinal tract. Aust N Z J Surg 1991; 61(1):35-7.
3. Tedeschi D. Intestinal obstruction caused by food foreign bodies. Minerva Med 1975; 66(68):3581-6.
4. Velitchkov NG. Ingested foreign bodies of the gastrointestinal tract: retrospective analysis of 542 cases. World J Surg 1996; 20(8): 1001-5.
5. Webb WA. Management of foreign bodies of the upper gastrointestinal tract. Gastroenterology 1988;94:204-16.
6. Ziter FM Jr. Intestinal perforation in adults due to ingested opaque foreign bodies . Am J Gastroenterol 1976; 66(4): 382-5.
7. Reddy S, Griffith G.S, Goldstein J, Stollman N. Toothpick Impaction with localized sigmoid perforation: successful colonoscopic management. Gastrointestinal Endoscopy Nov. 1999; vol 50 no. 5.
8. Guber MD, Suarez CA, Greve J. Toothpick perforation of the intestine diagnosed by a small bowel series. Am J Gastroenterol 1996;91:789-91.
9. Monkemuller KE, Patil R, Marino CR. Endoscopic removal of a toothpick from the transverse colon. Am J Gastroenterol 1996;91:2438-9.
10. Tenner S, Wong RC, Carr-Locke D, Davis SK, Farraye FA. Toothpick ingestion as a cause of acute and chronic duodenal inflammation. Am J Gastroenterol 1996;91:1860-2.
11. Meltzer SJ, Goldberg MD, Meltzer RM, Claps F. Appendiceal obstruction by a toothpick removed at colonoscopy. Am J Gastroenterol 1986;81:1107-8.
12. Cockerill FR, Wilson RW, Van Scoy RE. Traveling toothpicks. Mayo Clin Proc 1983;58:613-6.
13. Callon RA, Brady PG. Toothpick perforation of the sigmoid colon: an unusual case associated with Erysipelothrix rhusiopathiae septicemia. Gastrointest Endosc 1990;36:141-3.
14. Budnick LD. Toothpick related injuries in the United States, 1979-1982. JAMA 1984;252:796-7.
15. Schwartz TT, Graham DY. Toothpick perforation of the intestines. Ann Surg 1977;185:64-6.
16. Hashmi MA, Srinivas, Brimm C, et al. Toothpick perforation of the duodenum. J Clin Gastroenterol 1983;5:339-41.
17. Eisen G, Baron T, Dominitz J, et al. Guideline for the management of ingested foreign bodies. Gastrointestinal endoscopy. 2002; 55 (7).
18. Pinero, MA. Fernandez HA, Carrasco PM, Riquelme RJ, Parrila P. Intestinal perforation by foreign body. Eur J Surg 2000 Apr; 166(4):307-9.
19. McManus JE. Perforation of the intestine by ingested foreign bodies. Am J Surg 1941;53:393-402.